Case Report
Reversal of pure red cell aplasia by varicella zoster virus infection

Al-Anazi KA1*, Kanfar S1, Aldayel A2, Abduljalil O1 and Sayyed AH1
1Department of Hematology and Hematopoietic Stem Cell Transplantation, King Fahad Specialist Hospital, Dammam, Saudi Arabia
2Section of Hematopathology, Department of Pathology, King Fahad Specialist Hospital, Dammam, Saudi Arabia
*Address for Correspondence: Dr. Khalid Ahmed Al-Anazi, Consultant, Hemato Oncologist and Chairman, Department of Hematology and Hematopoietic Stem Cell Transplantation, Oncology Center, King Fahad Specialist Hospital, PO. Box: 15215, Dammam 31444, Saudi Arabia, Tel: 966-03-8431111; Fax: 966-13-8427420; Email: [email protected]
Dates: Submitted: 10 April 2019; Approved: 02 May 2019; Published: 03 May 2019
How to cite this article: Al-Anazi KA, Kanfar S, Aldayel A, Abduljalil O, Sayyed AH. Reversal of pure red cell aplasia by varicella zoster virus infection. J Hematol Clin Res. 2019; 3: 001-010. DOI: 10.29328/journal.jhcr.1001008
Copyright License: © 2019 Al-Anazi KA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Pure red cell aplasia; Bone marrow; Blood transfusion; Immunosuppressive therapy; Varicella zoster virus

Abstract
Background: Pure red cell aplasia is characterized by anemia, reticulocytopenia and diminished bone marrow erythroid precursors. It has multifactorial etiology and consequently several therapeutic interventions.
Case: In August 2017, a young patient was diagnosed to have pure red cell aplasia. She was given immunosuppressive therapy for approximately two months but this treatment was stopped due to intolerance. Later on she developed herpes zoster infection that was treated with valacyclovir. Subsequently, it was noted that the patient became blood transfusion independent due to normalization of her hemoglobin and regeneration of the erythroid precursors in the bone marrow.
Discussion: Varicella zoster virus behaves differently from other members of the herpes group of viruses such as cytomegalovirus and Epstein-Barr virus. Two retrospective studies, performed in patients with malignant hematological disorders and bone marrow failure, have shown that infection with the virus may cause stimulation of the three cell lines in the bone marrow and superior overall survival.
Conclusion: The outcome of the patient presented confirms the findings of the two studies showing long-term beneficial effects of varicella zoster virus infections in immunocompromised individuals.
Introduction
Pure red cell aplasia (PRCA) is a syndrome characterized by: severe normocytic normochromic anemia, severe reticulocytopenia, and marked reduction or absence of erythroid precursors in the bone marrow (BM) [1-4]. PRCA was first characterized by Kaznelson in the year 1922 [1,5]. The etiology and associations of PRCA are shown in table 1 [2-4,6-17].
| Table 1: Etiology and associations of pure red cell aplasia. |
| (1) Congenital, hereditary: Diamond-Blackfan anemia |
| (2) Acquired: |
| [a] Primary acquired: unknown cause; frequently antibody mediated with dysplastic morphologic abnormalities. |
| [b] Secondary acquired: |
| 1. Autoimmune and collagen vascular disorders: - Systemic lupus erythromatosis. |
| - Rheumatoid arthritis. |
| - Inflammatory bowel disease |
| - Myasthenia gravis |
| 2. Infections: - Viral: Parvovirus B-19; Hepatitis A and C; Mumps, Epstein-Barr virus; and Human immunodeficiency virus |
| - Tuberculosis. |
| - Group C Streptococci. |
| - Bacterial sepsis. |
| 3. Malignancy: - Lymphoproliferative disorders: Hodgkin's disease, and non-Hodgkin's lymphoma. |
| - Plasma cell disorders: multiple myeloma, and monoclonal gammopathy of unknown significance |
| - Myelodysplastic syndromes. |
| - Leukemia and myeloproliferative neoplasms: large granular lymphocyte leukemia, acute lymphoblastic leukemia, chronic myeloid leukemia, essential thrombocythemia, and primary myelofibrosis. |
| - Thymoma |
| - Other solid tumors |
| 4. Drugs: - Antimicrobials: chloramphenicol, ampicillin, linezolid, dapsone, and isoniazid. |
| - Anti-epileptics: phenytoin, and valproic acid. |
| - Immunosuppressive agents: azathioprine, mycophenolate mofetil, and tacrolimus. |
| - Novel therapies: lenalidomide, interleukin-2, tyrosine kinase inhibitors. |
| - Ani-erythropoietin antibodies. |
| - Drug abuse |
| 5- Hematopoietic stem cell transplantation: major ABO mismatching. |
| 6- Solid organ transplantation. |
| 7- Sickle cell disease. |
| 8- Pregnancy. |
Diamond-Blackfan anemia (DBA), the hereditary form of PRCA, is a rare congenital erythroid hypoplasia or inherited BM failure syndrome characterized by: (1) macrocytic anemia, (2) reticulocytopenia, (3) severely reduced numbers of erythroid precursors in the BM, (4) congenital malformations, and (5) predisposition to cancer [18-20]. DBA is a ribosomopathy where mutations in genes encoding ribosomal proteins or factors are involved in ribosomal biogenesis and more than 50% of patients have haploinsufficiency of either a small or large subunit associated ribosomal protein [18,19].
Dysregulation of T-cell mediated immunity is responsible for acquired PRCA [21]. Recurrent somatic mutations of signal transduction and activator of transcription 3 (STAT 3) have been reported in: T-cell large granular lymphocyte leukemia and chronic lymphoproliferative disorders of natural killer cells. However, mutations in STAT 3 gene have recently been reported with increased frequency in patients with PRCA [21-23]. Patients with positive STAT 3 mutations are usually younger in age and less responsive to cyclosporine-A therapy once compared to patients with negative STAT 3 mutational status [21].
The complications of PRCA include: (1) packed red blood cell (RBC) transfusion dependence particularly in chronic and relapsing cases; (2) evolution of: myelodysplastic syndrome (MDS), acute myeloid leukemia and aplastic anemia (AA); and (3) solid tumors such as: osteogenic sarcoma, colorectal cancer, breast carcinoma, squamous cell carcinoma, melanoma, non-Hodgkin lymphoma, female genital cancer, testicular carcinoma and lung cancer [19,24-28].
In patients with suspected PRCA, it is essential to have detailed history including family history as well as thorough physical examination. It is mandatory to rule out malignancy, autoimmune disorders and various infections [13,29-31]. The following viral infections are associated with BM suppression and anemia: cytomegalovirus, Epstein Barr virus, varicella zoster virus (VZV), parvovirus B-19, human herpes virus 6, in addition to hepatitis A and C viruses [32]. The diagnostic work-up of PRCA includes: complete blood count (CBC) and differential cell count; peripheral blood film; BM examination to differentiate PRCA from MDS, AA, and other forms of BM failure; cytogenetics, molecular mutational analysis and ribosomal studies; viral screens particularly parvovirus B-19, hepatitis and human immunodeficiency virus (HIV); and screen for malignancy [13,29-32].
There are several lines of treatment for PRCA. These therapeutic options vary considerably according to the cause and they range from supportive measures with blood transfusions as needed to more specific measures such as allogeneic hematopoietic stem cell transplantation (HSCT) as illustrated in table 2 [1-5,16-20,33-38]. The course and prognosis of PRCA vary depending on being hereditary or acquired and they depend on the underlying cause to a large extent [39-43]. However, most patients with chronic PRCA can be successfully treated with immunosuppressive therapies, but they require maintenance treatment with immunosuppressive agents [39-43]. Relapses and refractoriness to immunosuppression can be encountered [42]. The causes of death in patients with PRCA include: infectious complications, organ failure, associated cancer or BM failure as well as refractory and relapsing cases [39-43].
| Table 2: Therapeutic options in the management of pure red cell aplasia (PRCA) |
| 1- Treatment of the underlying disease such as lymphoma, leukemia and multiple myeloma with cytotoxic chemotherapy and novel agents. |
| 2- Withdrawal of the offending medication in case of drug-induced PRCA. |
| 3- Supportive measures: blood transfusions and iron chelation therapy. |
| 4- Intravenous immunoglobulins in case of parvovirus-induced PRCA. |
| 5- Immunosuppressive therapies: - Corticosteroids: prednisolone and high dose dexamethasone. - Cyclosporine-A. |
| - Cyclophosphamide. - Anti-thymocyte globulin. |
| 6- Monoclonal antibodies: rituximab, alemtuzumab, daclizumab, and daratumumab. |
| 7- Other drug therapies: - Interleukin-3 |
| - Valproic acid - Erythropoietin - Metoclopramide - Octreotide - Eltrombopag |
| 8- Plasmapheresis and donor lymphocyte infusions. |
| 9- Thymectomy and splenectomy. |
| 10- Allogeneic hematopoietic stem cell transplantation in case of Diamond-Blackfan anemia |
Case Presentation
In August 2017, a 34 year old Saudi female presented to King Fahad Specialist Hospital (KFSH) in Dammam, Saudi Arabia with anemic symptoms. She gave no history of any medical or surgical illness and she was not on any regular medication. Her family history was not contributory. Her physical examination at presentation showed: pallor but no jaundice, leg edema or external palpable lymphadenopathy. Her chest was clear and she had no abdominal tenderness or palpable organomegaly. Her cardiovascular and neurological examinations revealed no abnormality. Her CBC showed: white blood cell (WBC) count: 8.33×109/L, hemoglobin (Hb): 4.6 g/dL, platelet count: 407×109/L.
Differential cell count showed: 65% neutrophils, 24% lymphocytes and 8% monocytes. Peripheral blood film showed mild degree of macrocytosis, but no blasts or dysplastic changes. Renal, hepatic and coagulation profiles were all normal. BM examination showed: cellular marrow with normal myelopoiesis and megakaryopoiesis. However, the erythroid precursors were markedly reduced. There were no blasts or dysplastic changes (Figure 1). There was no cytogenetic abnormality. JAK 2 mutation was negative and paroxysmal nocturnal hemoglobinuria screen was negative. Thyroid function was normal. Serum vitamin B-12 and folate levels were normal. Hemoglobin electrophoresis and hemolytic screen were negative. Viral screens for cytomegalovirus, Epstein-Barr virus, parvovirus B-19 and HIV were all negative. Hepatitis A,B, and C screens were negative. Autoimmune and collagen vascular screens were also negative. Chest X-ray, electrocardiogram and ultrasound of the abdomen revealed no abnormality. Upper endoscopy with biopsies showed no evidence of gastritis, ulcers or malignancy.
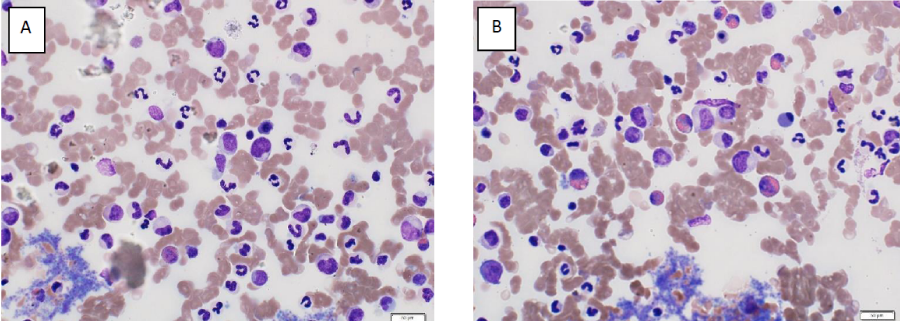
Figure 1A,B: Bone marrow aspirates prior to varicella zoster virus infection showing severe hypoplasia of the erythroid precursors.
Initially the patient was given packed RBC transfusions to relieve her symptoms. After establishing the diagnosis of PRCA and ruling out malignancy, autoimmune diseases and infections particularly with parvovirus B-19, the patient was commenced on the following immunosuppressive drugs: cyclosporine-A: 200 mg/kg orally twice daily and prednisolone: 1mg/kg/day. Two weeks after starting the immunosuppressive agents, Hb level improved but the patient remained packed RBC transfusion dependent. Unfortunately, she became intolerant to both medications to the extent that they were discontinued within 2 months of starting them. Two months after stopping cyclosporine-A and prednisolone, the patient had herpes zoster infection involving one dermatome over the right side of her chest wall. The diagnosis of herpes zoster infection was made on clinical grounds. Examination of vesicular fluid and scrapings of the skin lesions and the high titer of VZV-IgM antibodies confirmed the diagnosis of herpes zoster infection. The viral infection was treated with valacyclvir for 10 days. Unfortunately, the patient developed post-herpetic neuralgia that lasted for few months and was treated with analgesics and gabapentin.
Six weeks after the VZV infection, Hb level started to pick up gradually. Two months after the viral infection, not only Hb level became stable but also packed RBC transfusions were no longer required. Later on, the patient was kept on regular follow-up and her Hb level was noted to increase further as shown in table 3. Fourteen months after VZV infection, Hb level was 7 grams higher that that at the time of the viral infection (Table 3). BM examination was repeated and it showed complete regeneration of the erythroid precursors reflecting complete resolution of the PRCA (Figure 2). The patient was reassured, no new treatment was prescribed and she was kept on regular follow-up at the hematology outpatient clinic.
| Table 3: Shows the steady increase in hemoglobin level encountered following herpes zoster infection. |
|
| Time in relation to the viral infection | Hemoglobin level |
| 6 months before the viral infection (at diagnosis) |
4.6 g/dL |
| 4 months before the viral infection | 7.3 g/dL |
| 2 months before the viral infection | 7.9 g/dL |
| At the time of the viral infection | 7.6 g/dL |
| 2 months after the viral infection | 8.1 g/dL |
| 4 months after the viral infection | 8.4 g/dL |
| 6 months after the viral infection | 9.4 g/dL |
| 8 months after the viral infection | 10.3 g/dL |
| 10 months after the viral infection | 11.2 g/dL |
| 12 months after the viral infection | 12.3 g/dL |
| 14 months after the viral infection | 14.1 g/dL |
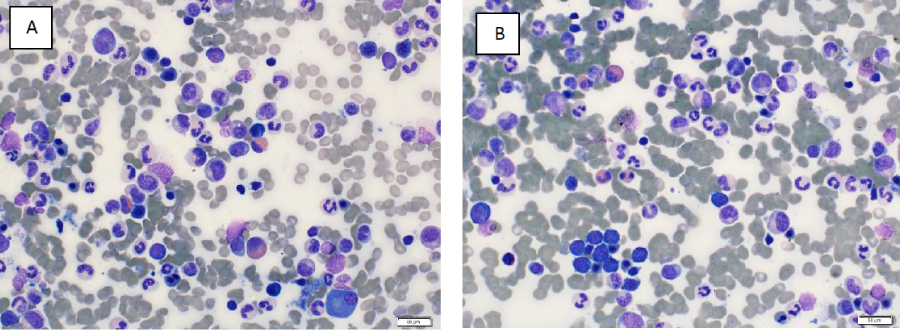
Figure 2A,B: Bone marrow aspirates showing resolution of the erythroid hypoplasia and regeneration of the erythroid precursors after recovery from varicella zoster virus infection.
Discussion
VZV is a double stranded DNA herpes virus. It is exclusively human virus and is highly contagious [44-46]. Primary VZV infection (chickenpox) occurs in childhood then the virus becomes latent in nerve ganglia [44,47]. Reactivation of the virus may occur decades later and causes herpes zoster which is manifested by typical painful skin eruption that has characteristic dermatomal distribution [44,47]. Reactivation of VZV is usually predisposed to by the following: (1) old age, male gender and AfroCaribbean descent; (2) comorbid medical conditions such as diabetes mellitus, chronic obstructive airway disease, end-stage renal disease and depression; and (3) immunosuppression due to: malignancy, autoimmune disorders, immunosuppressive therapies, trauma, cytotoxic chemotherapy, HSCT, and solid organ transplantation [44,47-49]. In severely immunocompromised individuals, particularly recipients of HSCT, preexisting antibodies do not prevent VZV reactivation but may contribute to decreased viral load thus resulting in mild clinical course [48]. Also, in immunocompromised patients having VZV infection: atypical skin eruption may be encountered and disseminated infection may occur in the absence of skin lesions [48,50].
Constitutional symptoms and prodromal manifestations such as fever, malaise and local pain usually occur and they are followed by the typical skin eruptions of both chickenpox and herpes zoster [44,47,49,51]. VZV infections may be complicated by: secondary bacterial infection, pneumonia, post-herpetic neuralgia, stroke and other vasculopathies, meningoencephalitis, segmental weakness and myelopathy, cranial neuropathies, giant cell arteritis, Guillain-Barre syndrome, enteric complications, severe local infection such as Ramsay Hunt syndrome, visceral and disseminated involvement, and death particularly in immunocompromised patients and complicated cases [44,47,49,50].
The diagnosis of VZV infection is usually made on clinical grounds based on the presence of the characteristic skin lesions [47,50]. However, additional diagnostic techniques include: (1) virus isolation by culture which carries a low yield rate, (2) serology using enzyme-linked immunosorbent assay, (3) direct fluorescent antibodies on scrapings obtained from active skin lesions, and (4) real-time polymerase chain reaction which has higher sensitivity than serological assays [47,50].
Therapeutic options for VZV infections include: (1) acyclovir which has been the standard of care for many years, and (2) valacyclovir, famcyclovir and bromovinyl deoxyuridine [52-54]. However, in immunocompromised individuals, high dose acyclovir is usually administered intravenously for 7-10 days [52-54]. However, for postherpetic neuralgia: gabapentin as well as local and systemic analgesics can be prescribed [53-56]. In patients with malignant hematological disorders (MHDs) receiving intensive chemotherapy and in recipients of various forms of HSCT, acyclovir prophylaxis is indicated and it has been shown to significantly reduce the rate of VZV infections in these severely immunocompromised patients [57]. Additionally, VZV vaccinations are usually offered to elderly individuals and to individuals at risk of contacting the infection [45,58-60].
Viruses have two opposing faces: (1) on the one side, they can cause harm and disease with early as well as late complications that carry significant morbidity and mortality and on rare occasions cellular transformation and cancer, and (2) on the other hand, viruses may provide hope to effectively treat several serious diseases [61]. Examples of the usefulness of certain viruses in the treatment of certain diseases include: use of viruses as vaccines; use of genetically engineered or naturally occurring viruses as anticancer agents in the setting of oncolytic virus therapy; and use of viruses as vectors in: induced pluripotent stem cells, gene therapy as well as chimeric antigen receptor T-cell therapy [61-64].
A single center, retrospective case controlled study included 16 episodes of VZV infection occurring in 14 patients with various types of MHDs and BM failure syndromes subjected to various forms of immunosuppressive therapies, cytotoxic chemotherapy and HSCT [54]. The study showed an increase in the 3 components of blood (WBC count, Hb level, and platelet count) starting approximately 6 weeks following VZV infection. This stimulation of the 3 hematopoietic cell lines in the BM that followed VZV infection was maintained for periods longer than 3 years post-VZV infection. The study clearly showed that VZV behaves differently from other members of the herpes group of viruses and can cause stimulation of BM activity starting 6 weeks after VZV infection and lasting for several years thereafter [54]. The authors postulated that immunological changes induced by VZV infection particularly cytokine release could be responsible for the stimulation of BM activity by VZV infection [54].
Another single center retrospective study included 191 patients with multiple myeloma (MM) treated initially with cytotoxic chemotherapy, bortezomib-based or thalidomide-based therapy then subjected to high dose melphalan followed by autologous HSCT [65]. Approximately 30% of these patients developed VZV infections either before or after HSCT. VZV infections were encountered more frequently in patients with: advanced stage of disease, renal failure and relapsing MM [65]. Despite encountering VZV infections in patients with worse expected prognosis, the overall survival in patients who developed VZV infection was superior to that in patients who never developed the infection. Additionally, there was no delay in neutrophil recovery post-HSCT in patients infected with VZV and platelet count recovery post-HSCT occurred earlier in patients infected with VZV [65].
The patient reported remained blood transfusion dependent for months after the diagnosis of PRCA. The immunosuppressive therapy improved her Hb level but never abolished the need for blood transfusions. Unfortunately, the patient developed intolerance to cyclosporine-A and prednisolone treatments that were stopped 2 months after commencing these drugs. Development of herpes zoster infection complicated by postherpetic neuralgia did not allow resumption of the combined immunosuppressive therapy. The stabilization of Hb level then the subsequent and gradual increase encountered in Hb level encouraged us and the patient not to have any new therapy started. The documentation of the recovery of erythroid precursors in the BM was reassuring that no further treatment would be needed.
Conclusion and Recommandations
The recovery of red cell aplasia with normalization of Hb level months following VZV infection in the patient reported together with the results of the 2 retrospective studies, discussed above, which showed clear evidence of stimulation of BM activity and superior outcome of immunocompromised patients infected with VZV should encourage scientists and researchers to give this potentially useful virus enough attention. The effects of VZV on BM activity and on diseases such as BM failure syndromes and MHDs through direct or indirect immunological mechanisms merit thorough investigations. The virus itself or the serum obtained from patients infected with VZV may ultimately become valuable tools in the management of patients with various BM failure syndromes or MHDs.
Acknowledgment
We are grateful to all medical, nursing and technical staff at KFSH in Dammam, Saudi Arabia who took care of the patient presented.
References
- Sawada K, Fujishima N, Hirokawa M. Acquired pure red cell aplasia: updated review of treatment. Br J Haematol. 2008; 142: 505-514. Ref.: https://tinyurl.com/y24mg42v
- Means RT Jr. Pure red cell aplasia. Blood. 2016; 128: 2504- 2509. Ref.: https://tinyurl.com/y4wjzkf5
- Means RT Jr. Pure red cell aplasia. Hematology Am Soc Hematol Educ Program. 2016; 2016: 51-56. Ref.: https://tinyurl.com/y28ta36n
- Schrier SL. Acquired pure red cell aplasia in the adult. Edited by: Mentzer WC, Tirnauer JS. Up To Date. 2019; Ref.: https://tinyurl.com/y3facpmq
- Crabol Y, Terrier B, Rozenberg F, Pestre V, Legendre C, et al. Groupe d'experts de l'Assistance Publique-Hôpitaux de Paris. Intravenous immunoglobulin therapy for pure red cell aplasia related to human parvovirus B19 infection: a retrospective study of 10 patients and review of the literature. Clin Infect Dis. 2013; 56: 968-977. Ref.: https://tinyurl.com/y65gru7m
- Ito T, Nakaya A, Fujita S, Satake A, Nakanishi T, et al. Secondary pure red cell aplasia in multiple myeloma treated with lenalidomide. Leuk Res Rep. 2018; 10: 4-6. Ref.: https://tinyurl.com/y5r94vu7
- Sawlani KK, Chaudhary SC, Singh J, Raja DC, Mishra S, et al. Dapsone-induced pure red cell aplasia and cholestatic jaundice: A new experience for diagnosis and management. J Res Pharm Pract. 2016; 5: 215-218. Ref.: https://tinyurl.com/y3tt5dhh
- Liang TB, Li DL, Yu J, Bai XL, Liang L, et al. Pure red cell aplasia due to parvovirus B19 infection after liver transplantation: a case report and review of the literature. World J Gastroenterol. 2007; 13: 2007-2010. Ref.: https://tinyurl.com/y5rkl9bk
- Saito Y, Sawada Y, Koga Y, Sunaga N, Tsukagoshi Y, et al. Isoniazid-induced pure red cell aplasia in a patient with sarcoidosis: a patient summary and review of the literature. Intern Med. 2017; 56: 2753-2757. Ref.: https://tinyurl.com/y3852u2v
- Dutcher JP, Fan W, Wiernik PH. Pure red cell aplasia following interleukin-2 therapy. J Investig Med High Impact Case Rep. 2016; 4: 324709616643991. Ref.: https://tinyurl.com/y3zb2kcf
- Poudyal BS, Tuladhar S, Gyawali B. TKI-induced pure red cell aplasia: first case report of pure red cell aplasia with both imatinib and nilotinib. ESMO Open. 2016; 1: e000058. Ref.: https://tinyurl.com/y2ryzjug
- Luo Z, Xu N, Wang Y, Huang X, Cao C, et al. Linezolid-induced pure red cell aplasia: a case report and literature review. J Int Med Res. 2018; 46: 4837-4844. Ref.: https://tinyurl.com/y5hceksh
- Balikar R, Redkar NN, Patil MA, Pawar S. Myasthenia gravis and pure red cell aplasia: a rare association. BMJ Case Rep. 2013; 2013. pii: bcr2012008224. Ref.: https://tinyurl.com/y2y83xpa
- Bennett CL, Luminari S, Nissenson AR, Tallman MS, Klinge SA, et al. Pure red-cell aplasia and epoetin therapy. N Engl J Med. 2004; 351: 1403-1408. Ref.: https://tinyurl.com/yxj9d332
- Sekiguchi Y, Shimada A, Imai H, Wakabayashi M, Sugimoto K, et al. A case of recurrent autoimmune hemolytic anemia during remission associated with acute pure red cell aplasia and hemophagocytic syndrome due to human parvovirus B19 infection successfully treated by steroid pulse therapy with a review of the literature. Int J Clin Exp Pathol. 2014; 7: 2624-2635. Ref.: https://tinyurl.com/y56ccbcn
- Balasubramanian SK, Sadaps M, Thota S, Aly M, Przychodzen BP, et al. Rational management approach to pure red cell aplasia. Haematologica. 2018; 103: 221-230. Ref.: https://tinyurl.com/yxlcmuq2
- Sharma VR, Fleming DR, Slone SP. Pure red cell aplasia due to parvovirus B19 in a patient treated with rituximab. Blood. 2000; 96: 1184-1186. Ref.: https://tinyurl.com/y38xzcau
- Lipton JM, Ellis SR. Diamond-Blackfan anemia: diagnosis, treatment, and molecular pathogenesis. Hematol Oncol Clin North Am. 2009; 23: 261-282. Ref.: https://tinyurl.com/y5sc9kkj
- Vlachos A, Muir E. How I treat Diamond-Blackfan anemia. Blood. 2010; 116: 3715-3723. Ref.: https://tinyurl.com/yyd6tgrl
- Sjögren SE, Flygare J. Progress towards mechanism-based treatment for Diamond-Blackfan anemia. Sci World J. 2012; 2012: 184362. Ref.: https://tinyurl.com/y27amr3a
- Kawakami T, Sekiguchi N, Kobayashi J, Imi T, Matsuda K, et al. Frequent STAT3 mutations in CD8+ T cells from patients with pure red cell aplasia. Blood Adv. 2018; 2: 2704-2712. Ref.: https://tinyurl.com/y5pklsew
- Ishida F, Matsuda K, Sekiguchi N, Makishima H, Taira C, et al. STAT3 gene mutations and their association with pure red cell aplasia in large granular lymphocyte leukemia. Cancer Sci. 2014; 105: 342-346. Ref.: https://tinyurl.com/y6h3jdpu
- Qiu ZY, Fan L, Wang L, Qiao C, Wu YJ, et al. STAT3 mutations are frequent in T-cell large granular lymphocytic leukemia with pure red cell aplasia. J Hematol Oncol. 2013; 6: 82. Ref.: https://tinyurl.com/y2o894bn
- Savage SA, Dufour C. Classical inherited bone marrow failure syndromes with high risk for myelodysplastic syndrome and acute myelogenous leukemia. Semin Hematol. 2017; 54:105-114. Ref.: https://tinyurl.com/y2t7o8wb
- Kim HD, Kim KW, Park SY, Ko HJ, An YY, et al. Myelodysplastic syndrome with erythroid aplasia following pure red cell aplasia. Korean J Intern Med. 2004; 19: 193-195. Ref.: https://tinyurl.com/y67qpjhd
- Lipton JM, Federman N, Khabbaze Y, Schwartz CL, Hilliard LM, et al. Diamond-Black Anemia Registry. Osteogenic sarcoma associated with Diamond-Blackfan anemia: a report from the Diamond-Blackfan Anemia Registry. J Pediatr Hematol Oncol. 2001; 23: 39-44. Ref.: https://tinyurl.com/y3qqjznu
- Matsuda I, Tsuchida YA, Toyoshima F, Tozawa K, Ikehara H, et al. Occurrence of colon tumors in a 16-year-old Japanese boy after hematopoietic stem cell transplantation for Diamond Blackfan anemia at age of 4: a case report. Int J Clin Exp Pathol. 2015; 8: 5938-5943. Ref.: https://tinyurl.com/yxrpq7az
- Bannon SA, DiNardo CD. Hereditary predispositions to myelodysplastic syndrome. Int J Mol Sci. 2016; 17. pii: E838. Ref.: https://tinyurl.com/y27ucy5o
- Garewal G, Ahluwalia J, Das R, Marwaha RK. Parvovirus B19associated transient red cell aplasia in children: the role of bone marrow examination in unusual presentations. Pediatr Hematol Oncol. 2004; 21: 505-511. Ref.: https://tinyurl.com/yyk3bjl6
- Lin CS, Yu YB, Hsu HS, Chou TY, Hsu WH, et al. Pure red cell aplasia and hypogammaglobulinemia in a patient with thymoma. J Chin Med Assoc. 2009; 72: 34-38. Ref.: https://tinyurl.com/y2lnnq7b
- Kanellopoulos A, Koutsi K, Georgiou G, Ntalagiorgos T, Petevi K, et al. Pure red cell aplasia complicating the course of long-standing mantle cell lymphoma. Int J Hematol. 2014; 99: 777-781. Ref.: https://tinyurl.com/yxjr6ayz
- Morinet F, Leruez-Ville M, Pillet S, Fichelson S. Concise review: Anemia caused by viruses. Stem Cells. 2011; 29: 1656-1660. Ref.: https://tinyurl.com/y4f4samu
- Au WY, Lam CC, Chim CS, Pang AW, Kwong YL. Alemtuzumab induced complete remission of therapy-resistant pure red cell aplasia. Leuk Res. 2005; 29: 1213-1215. Ref.: https://tinyurl.com/yyafyq7l
- He GS, Zhang X, Wu DP, Sun AN, Miao M, et al. Retreatment with fludarabine and cyclosporine for one case of refractory pure red cell aplasia. Chin Med Sci J. 2008; 23: 60-62. Ref.: https://tinyurl.com/y6yfm9p3
- Messner HA, Fauser AA, Curtis JE, Dotten D. Control of antibody-mediated pure red-cell aplasia by plasmapheresis. N Engl J Med. 1981; 304: 1334-1338. Ref.: https://tinyurl.com/y57dlb8g
- Palmieri G, Lastoria S, Colao A, Vergara E, Varrella P, et al. Successful treatment of a patient with a thymoma and pure red-cell aplasia with octreotide and prednisone. N Engl J Med. 1997; 336: 263-265. Ref.: https://tinyurl.com/y4jb7nc5
- Eisemann G, Damesheq W. Splenectomy for pure red-cell hypoplastic (aregenerative) anemia associated with autoimmune hemolytic disease; report of a case. N Engl J Med. 1954; 251: 1044-1048. Ref.: https://tinyurl.com/yxql7g74
- McGuire WA, Yang HH, Bruno E, Brandt J, Briddell R, et al. Treatment of antibody-mediated pure red-cell aplasia with high-dose intravenous gamma globulin. N Engl J Med. 1987; 317: 1004-1008. Ref.: https://tinyurl.com/y2rqt5l3
- Hirokawa M. Progress in the clinical management of pure red cell aplasia and future prospects. Rinsho Ketsueki. 2016; 57: 110-116. Ref.: https://tinyurl.com/y4hsjtwg
- Castelli R, Vismara A, Pavia G, Dagani R, Porro T. Relapsing pure red cell aplasia associated with B-cell chronic lymphocytic leukemia successfully treated by intravenous immunoglobulin concentrate. Ann Ital Med Int. 2002; 17: 47-50. Ref.: https://tinyurl.com/yxf34n22
- Kurtzman G, Frickhofen N, Kimball J, Jenkins DW, Nienhuis AW, et al. Pure red-cell aplasia of 10 years' duration due to persistent parvovirus B19 infection and its cure with immunoglobulin therapy. N Engl J Med. 1989; 321: 519-523. Ref.: https://tinyurl.com/y6lgcmkg
- Koduri PR, Kumapley R, Valladares J, Teter C. Chronic pure red cell aplasia caused by parvovirus B19 in AIDS: use of intravenous immunoglobulin--a report of eight patients. Am J Hematol. 1999; 61: 16-20. Ref.: https://tinyurl.com/yxjxtjlp
- Hirokawa M, Sawada K, Fujishima N, Teramura M, Bessho M, et al. Long-term outcome of patients with acquired chronic pure red cell aplasia (PRCA) following immunosuppressive therapy: a final report of the nationwide cohort study in 2004/2006 by the Japan PRCA collaborative study group. Br J Haematol. 2015; 169: 879-886. Ref.: https://tinyurl.com/y26e2mu5
- Kennedy PGE, Gershon AA. Clinical features of varicella-zoster virus infection. Viruses. 2018; 10. pii: E609. Ref.: https://tinyurl.com/y4tc4l38
- Weber DJ. Prevention and control of varicella-zoster virus in hospitals. Edited by: Hirsch MS, Mitty JM. Up To Date 2019. Ref.: https://tinyurl.com/yyp2jpre
- Cohrs RJ, Gilden DH, Mahalingam R. Varicella zoster virus latency, neurological disease and experimental models: an update. Front Biosci. 2004; 9: 751-762. Ref.: https://tinyurl.com/y6dwn4v4
- Albrecht MA, Levin MJ. Epidemiology, clinical manifestations and diagnosis of herpes zoster. Edited by: Hirsch MS, Mitty J. Up To Date. 2019; Ref.: https://tinyurl.com/y4l2cbfg
- Onozawa M, Hashino S, Takahata M, Fujisawa F, Kawamura T, et al. Relationship between preexisting anti-varicella-zoster virus (VZV) antibody and clinical VZV reactivation in hematopoietic stem cell transplantation recipients. J Clin Microbiol. 2006; 44: 4441-4443. Ref.: https://tinyurl.com/yxu2vhkd
- Cvjetković D, Jovanović J, Hrnjaković-Cvjetković I, Brkić S, Bogdanović M. Reactivation of herpes zoster infection by varicellazoster virus. Med Pregl. 1999; 52: 125-128. Ref.: https://tinyurl.com/y6atj2b4
- Albrecht MA. Diagnosis of varicella zoster virus infection. Edited by: Hirsch MS, Mitty JM. Up To Date. 2019; Ref.: https://tinyurl.com/y4ykxdbw
- Erskine N, Tran H, Levin L, Ulbricht C, Fingeroth J, et al. A systematic review and meta-analysis on herpes zoster and the risk of cardiac and cerebrovascular events. PLoS One. 2017; 12: e0181565. Ref.: https://tinyurl.com/yxv3wtg2
- Breuer J, Whitley R. Varicella zoster virus: natural history and current therapies of varicella and herpes zoster. Herpes. 2007; 14 Suppl 2: 25-29. Ref.: https://tinyurl.com/y4293sbo
- Mustafa MB, Arduino PG, Porter SR. Varicella zoster virus: review of its management. J Oral Pathol Med. 2009; 38: 673-688. Ref.: https://tinyurl.com/y4cja5al
- Al-Anazi KA, Al-Jasser AM, Evans DA. Effect of varicella zoster virus infection on bone marrow function. Eur J Haematol. 2005; 75: 234-240. Ref.: https://tinyurl.com/y2c9rbum
- Kim SR, Khan F, Ramirez-Fort MK, Downing C, Tyring SK. Varicella zoster: an update on current treatment options and future perspectives. Expert Opin Pharmacother. 2014; 15: 61-71. Ref.: https://tinyurl.com/yxhzcekw
- Johnson RW. Herpes zoster in the immunocompetent patient: management of post-herpetic neuralgia. Herpes. 2003; 10: 38-45. Ref.: https://tinyurl.com/y6ezyjnx
- Wada-Shimosato Y, Tanoshima R, Hiratoko K, Takeuchi M, Tsujimoto SI, et al. Effectiveness of acyclovir prophylaxis against varicella zoster virus disease after allogeneic hematopoietic cell transplantation: a systematic review and meta-analysis. Transpl Infect Dis. 2019; e13061. Ref.: https://tinyurl.com/yxom486h
- Wang L, Zhu L, Zhu H. Efficacy of varicella (VZV) vaccination: an update for the clinician. Ther Adv Vaccines. 2016; 4: 20-31. Ref.: https://tinyurl.com/y6jdwxqh
- Harada K, Heaton H, Chen J, Vazquez M, Meyer J. Zoster vaccine-associated primary varicella infection in an immunocompetent host. BMJ Case Rep. 2017; 2017. pii: bcr-2017-221166. Ref.: https://tinyurl.com/yywmryxu
- Gabutti G, Bonanni P, Conversano M, Fanelli G, Franco E, et al. Prevention of herpes zoster and its complications: from clinical evidence to real life experience. Hum Vaccin Immunother. 2017; 13: 391-398. Ref.: https://tinyurl.com/yxvd7ehv
- Belcaid Z, Lamfers ML, van Beusechem VW, Hoeben RC. Changing faces in virology: the Dutch shift from oncogenic to oncolytic viruses. Hum Gene Ther. 2014; 25: 875-884. Ref.: https://tinyurl.com/yywhme9z
- Fukuhara H, Ino Y, Todo T. Oncolytic virus therapy: a new era of cancer treatment at dawn. Cancer Sci. 2016 Oct; 107: 1373-1379. Ref.: https://tinyurl.com/y53r79zc
- Ajina A, Maher J. Prospects for combined use of oncolytic viruses and CAR T-cells. J Immunother Cancer. 2017; 5: 90. Ref.: https://tinyurl.com/y4gwuezv
- Howells A, Marelli G, Lemoine NR, Wang Y. Oncolytic virusesinteraction of virus and tumor cells in the battle to eliminate cancer. Front Oncol. 2017; 7: 195. Ref.: https://tinyurl.com/yykeu2ht
- Kamber C, Zimmerli S, Suter-Riniker F, Mueller BU, Taleghani BM, et al. Varicella zoster virus reactivation after autologous SCT is a frequent event and associated with favorable outcome in myeloma patients. Bone Marrow Transplant. 2015; 50: 573-578. Ref.: https://tinyurl.com/yxuxmp7t