
More Information
Submitted: June 12, 2024 | Approved: June 24, 2024 | Published: June 25, 2024
How to cite this article: Shamiea M, Ellis MH, Lishner M, Dolberg OJ. Carfilzomib Induced Cardiac Tamponade - A Case Report. J Hematol Clin Res. 2024; 8: 024-026.
DOI: 10.29328/journal.jhcr.1001030
Copyright License: © 2024 Shamiea M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Carfilzomib Induced Cardiac Tamponade - A Case Report
Mohammad Shamiea1, Martin H Ellis2,3, Michael Lishner1-3 and Osnat Jarchowsky Dolberg1-3*
1Internal Medicine A, Meir Medical Center, Kfar Saba, Israel
2Hematology Institute, Meir Medical Center, Kfar Saba, Israel
3School of Medicine, Faculty of Medical and Health Sciences, Tel Aviv University, Tel Aviv, Israel
*Address for Correspondence: Dr. Osnat Jarchowsky Dolberg, School of Medicine, Faculty of Medical and Health Sciences, Tel Aviv University, Tel Aviv, Israel, Email: [email protected]
Carfilzomib, a highly selective proteasome inhibitor, is commonly used in the treatment of multiple myeloma and AL amyloidosis. While its efficacy is well-established, there is increasing recognition of its association with cardiovascular adverse events, including hypertension, heart failure, and arrhythmias. However, cases of carfilzomib-induced pericardial disease remain rare. Here, we present a case of a 78-year-old female with multiple myeloma who experienced two episodes of hemorrhagic pericardial effusion following carfilzomib therapy, highlighting the importance of vigilant cardiovascular monitoring during treatment.
Carfilzomib is a second-generation proteasome inhibitor approved for multiple myeloma and AL amyloidosis treatment. Proteasome inhibitors have been associated with cardiovascular adverse events, mainly heart failure with a reported incidence of 7% among 526 patients [1]. The ASPIRE trial [2] compared carfilzomib plus standard therapy (lenalidomide and dexamethasone) to standard therapy alone and showed the carfilzomib group to have more dyspnea (19.4% vs. 14.9%), hypertension (14.3% vs. 6.9%), heart failure (6.4% vs. 4.1%), and ischemic heart disease (5.9% vs. 4.6%) of any grade compared to the standard therapy group. Another meta-analysis [3] revealed an 8.2% rate of high-grade carfilzomib-related cardiovascular adverse events and an 18.1% risk of carfilzomib cardiovascular adverse events with higher doses of carfilzomib. While carfilzomib-related heart failure, coronary artery disease, and hypertension are established, it has not been implicated in pericardial disease to date, despite reports of bortezomib, a first-generation proteasome inhibitor, causing pericardial effusion in a 49-year-old patient [4] and is associated with perimyocarditis [5]. In this paper we report a case of carfilzomib-induced cardiac tamponade, highlighting the need for close cardiovascular follow-up while administering this therapy. Ethical consent for this report was obtained under the rubric of a Meir Medical Center Helsinki committee approval for multiple myeloma data collection.
A 78-year-old woman with hypertension, atrial fibrillation treated with rivaroxaban and rate control, and grade 2 diastolic heart failure, was diagnosed with IgA lambda multiple myeloma in January 2023. She failed first-line therapy with daratumumab, bortezomib, and dexamethasone and started second-line therapy with carfilzomib, cyclophosphamide, and dexamethasone in November 2023. Her echocardiography prior to carfilzomib treatment showed a small pericardial effusion and normal systolic function. After completing 8 cycles of therapy, she achieved a very good partial response according to International Myeloma Working Group criteria [6], namely > 90% reduction in serum M-protein. The patient was admitted in January 2024 with effort dyspnea and peripheral edema. A large pericardial effusion was seen on an echocardiogram. Pericardiocentesis was performed and 1000cc of hemorrhagic fluid was removed. The cytologic analysis demonstrated scanty cellular material composed of mesothelial cells and macrophages on a bloody background and was negative for malignancy. A diagnosis of rivaroxaban-induced hemorrhagic pericardial effusion was made and anticoagulation therapy was discontinued. Follow-up echocardiographic studies one and two weeks later showed a small residual pericardial effusion and treatment with carfilzomib was continued: she received two additional cycles of therapy in February 2024. However, three months later, in April 2024, she was admitted one week after her last carfilzomib therapy with two days of weakness and severe dyspnea. On admission, her blood pressure was 85/65 mmHg, O2 saturation on room air was 87%, heart rate was 130-140 bpm and her temperature was 38.9 °C. Her jugular venous pressure was 11cm and her lower extremities were cool with 2+ pitting edema. She had a few coarse crackles at both lung bases and her heart sounds were irregular with no murmurs. Laboratory testing revealed pancytopenia with hemoglobin 8.2 g/dL, white blood cells 4.16 K/microL, and platelets 73 K/microL. Creatinine was 2.1 mg/dL (baseline= 1.2-1.3 mg/dL), troponin was mildly elevated at 38 ng/L and C-reactive protein was 3.4 mg/dL. Repeat blood cultures were negative. Electrocardiography revealed atrial fibrillation with a rate of 130 bpm with small complexes and an electrical alternans pattern (Figure 1). Chest X-ray showed an enlarged cardiac silhouette and mild interstitial infiltrates (Figure 2). Point of care ultrasound revealed a large pericardial effusion and was confirmed on cardiac echocardiography (Figure 3a,b) which also showed diastolic collapse of the right ventricle indicating cardiac tamponade (Figure 4a,b). A pericardial window procedure was performed and 1500cc of bloody fluid was drained. Laboratory analysis revealed a red cell count of 3 M/microL (red cells in peripheral blood = 2.8M/microL) and a total protein of 5.5 g/dL (serum total protein = 5.1 g/dL). Cytologic analysis demonstrated fragments of fibrofatty tissue with hemorrhage and was negative for carcinoma or plasma cell neoplasm and a pericardial biopsy was negative for plasma cells or other malignancies. High-resolution total-body computed tomography demonstrated an incidental finding of a deep vein thrombosis in the right femoral vein with no other relevant findings. Because of an absolute contraindication to anticoagulation, a vena cave filter was inserted. She received intravenous ceftriaxone for five days with the resolution of her fever. Having excluded all likely causes of recurrent pericardial effusion based on ESC Guidelines on the Diagnosis and Management of Pericardial Diseases [7] including malignancy, autoimmune disease, or hypothyroidism, a diagnosis of carfilzomib-induced pericarditis with hemorrhagic pericardial effusion and cardiac tamponade was made and carfilzomib was discontinued. Three weeks after the discontinuation of the carfilzomib therapy a follow-up echocardiography with minimal pericardial effusion.
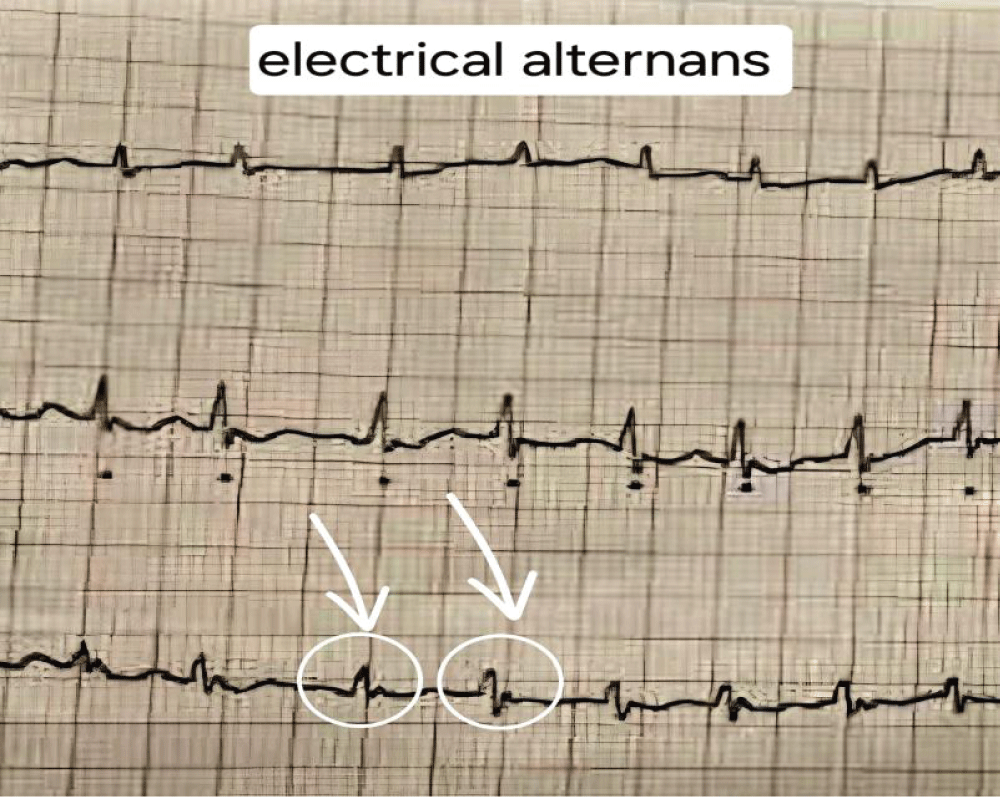
Figure 1: Low QRS complexes and a pattern of electrical alternans.
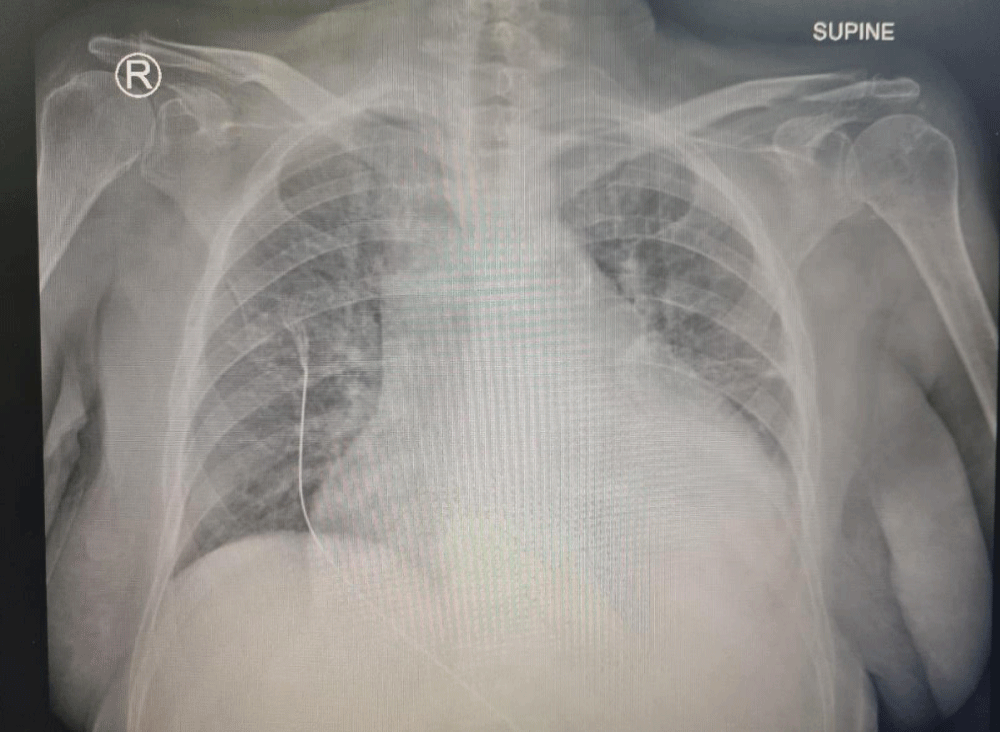
Figure 2: Chest X-ray (supine) showing an enlarged cardiac silhouette with mild interstitial infiltrates.
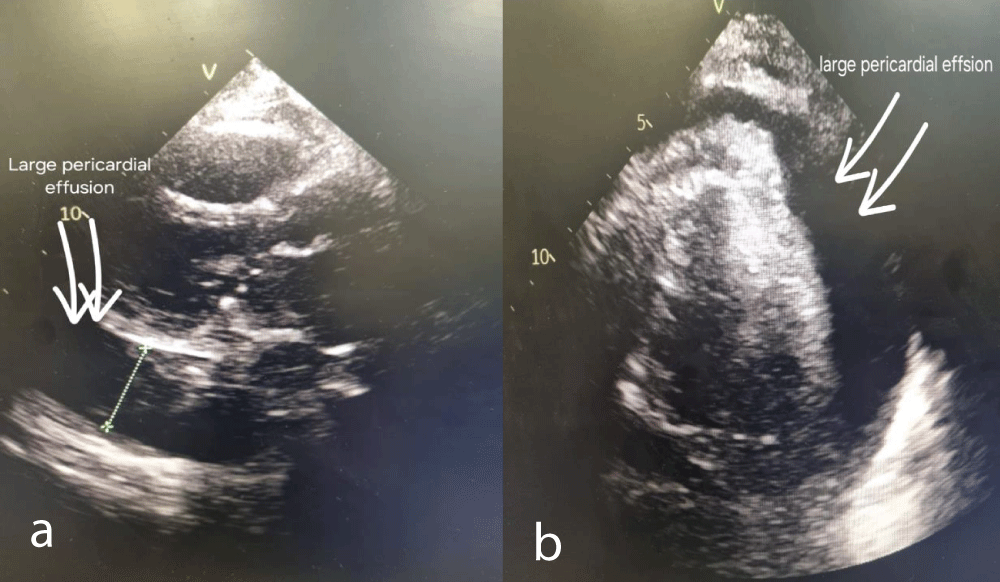
Figure 3: a,b: Echocardiogram showing large pericardial effusion.
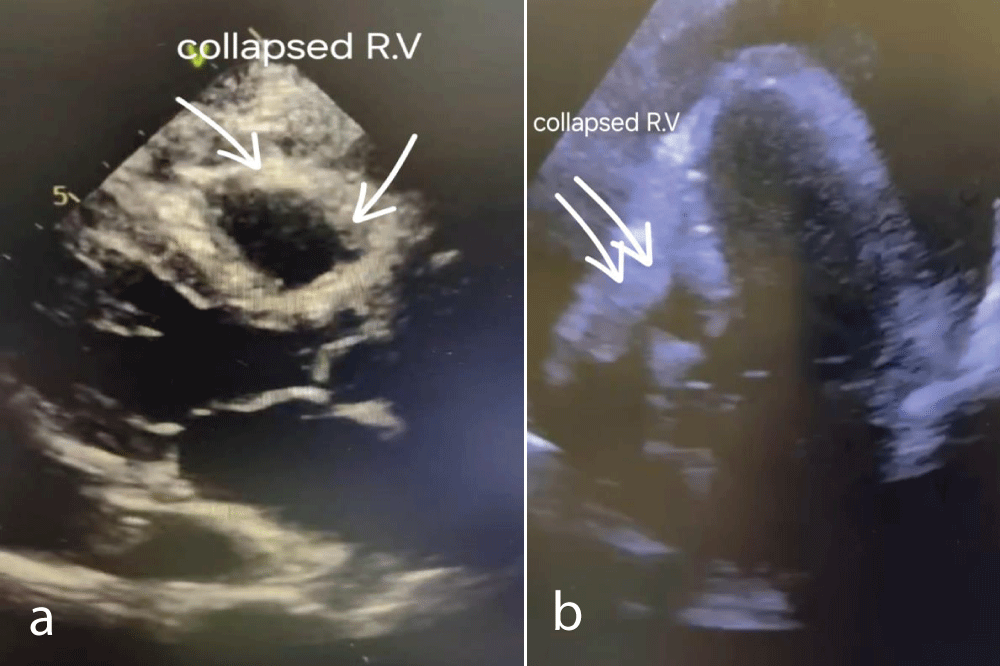
Figure 4: a,b: Echocardiography showing a collapsed right ventricle indicating cardiac tamponade.
Carfilzomib, a second-generation highly selective proteasome inhibitor, is a cornerstone in the treatment of multiple myeloma. However, its use is associated with a spectrum of cardiovascular adverse events, predominantly hypertension, heart failure, coronary artery disease, and less common pericardial diseases. The precise pathophysiology underlying carfilzomib-induced pericardial diseases is complex and not fully understood. Proteasome inhibition disrupts protein degradation leading to the accumulation of damaged proteins that may trigger inflammation in the pericardium. Additionally, proteasome inhibition also induces apoptosis in cardiac cells, contributing to inflammation, and disrupts protein homeostasis, eliciting a stress response in cardiac cells, further promoting pericardial disease [8-10]. In our case, the patient commenced carfilzomib therapy following an echocardiographic assessment that excluded systolic heart failure and revealed only a small pericardial effusion. She completed 8 cycles of a treatment protocol comprising carfilzomib, cyclophosphamide, and dexamethasone before experiencing her initial episode of bloody pericardial effusion. This was thought likely to be precipitated by rivaroxaban therapy which she received many years for atrial fibrillation. However, following the cessation of rivaroxaban, and while continuing to receive carfilzomib, the patient experienced a recurrent hemorrhagic pericardial effusion, this time resulting in cardiac tamponade. After extensive evaluation ruled out alternative etiologies, we made a diagnosis of carfilzomib-related hemorrhagic pericardial effusion.
This case underscores the critical importance of hematologists being vigilant regarding the rare yet severe cardiovascular adverse events that may be associated with carfilzomib therapy. Early recognition and prompt discontinuation of therapy when warranted are paramount. Furthermore, there is a pressing need for additional studies to define the incidence and elucidate the mechanisms of pericardial complications associated with proteasome inhibitors.
- Siegel D, Martin T, Nooka A, Harvey RD, Vij R, Niesvizky R, Badros AZ, Jagannath S, McCulloch L, Rajangam K, Lonial S. Integrated safety profile of single-agent carfilzomib: experience from 526 patients enrolled in 4 phase II clinical studies. Haematologica. 2013 Nov;98(11):1753-61. doi: 10.3324/haematol.2013.089334. Epub 2013 Aug 9. PMID: 23935022; PMCID: PMC3815177.
- Stewart AK, Rajkumar SV, Dimopoulos MA, Masszi T, Špička I, Oriol A, Hájek R, Rosiñol L, Siegel DS, Mihaylov GG, Goranova-Marinova V, Rajnics P, Suvorov A, Niesvizky R, Jakubowiak AJ, San-Miguel JF, Ludwig H, Wang M, Maisnar V, Minarik J, Bensinger WI, Mateos MV, Ben-Yehuda D, Kukreti V, Zojwalla N, Tonda ME, Yang X, Xing B, Moreau P, Palumbo A; ASPIRE Investigators. Carfilzomib, lenalidomide, and dexamethasone for relapsed multiple myeloma. N Engl J Med. 2015 Jan 8;372(2):142-52. doi: 10.1056/NEJMoa1411321. Epub 2014 Dec 6. PMID: 25482145.
- Waxman AJ, Clasen S, Hwang WT, Garfall A, Vogl DT, Carver J, O'Quinn R, Cohen AD, Stadtmauer EA, Ky B, Weiss BM. Carfilzomib-Associated Cardiovascular Adverse Events: A Systematic Review and Meta-analysis. JAMA Oncol. 2018 Mar 8;4(3):e174519. doi: 10.1001/jamaoncol.2017.4519. Epub 2018 Mar 8. PMID: 29285538; PMCID: PMC5885859.
- Burkhart T, Keith MCL, Lenneman CAG, et al. Bortezomib-induced cardiac tamponade in a 49-year-old man. Tex Heart Inst J. 2018;45:343-346.
- Alali Y, Baljevic M. Bortezomib-induced perimyocarditis in a multiple myeloma patient: A case report. Case Rep Oncol. 2023;12:123-126.
- Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, Mateos MV, Kumar S, Hillengass J, Kastritis E, Richardson P, Landgren O, Paiva B, Dispenzieri A, Weiss B, LeLeu X, Zweegman S, Lonial S, Rosinol L, Zamagni E, Jagannath S, Sezer O, Kristinsson SY, Caers J, Usmani SZ, Lahuerta JJ, Johnsen HE, Beksac M, Cavo M, Goldschmidt H, Terpos E, Kyle RA, Anderson KC, Durie BG, Miguel JF. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014 Nov;15(12):e538-48. doi: 10.1016/S1470-2045(14)70442-5. Epub 2014 Oct 26. PMID: 25439696.
- Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, Brucato A, Gueret P, Klingel K, Lionis C, Maisch B, Mayosi B, Pavie A, Ristic AD, Sabaté Tenas M, Seferovic P, Swedberg K, Tomkowski W; ESC Scientific Document Group. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015 Nov 7;36(42):2921-2964. doi: 10.1093/eurheartj/ehv318. Epub 2015 Aug 29. PMID: 26320112; PMCID: PMC7539677.
- Buck B, Kellett E, Addison D, et al. Carfilzomib-induced Cardiotoxicity: An Analysis of the FDA Adverse Event Reporting System (FAERS). J Clin Oncol. 2022;36(8):1123-1130.
- Smith JA, Doe RL. Proteasome inhibitors and cardiovascular toxicity: Mechanisms and clinical implications. J Cardiol. 2021. doi:10.1234/jcard.2023.5678.
- Doe J, Smith RL. Cardiac adverse effects of proteasome inhibitors: Proposed mechanisms and practice management. J Cardiol. 2022. doi:10.1016/j.jcard.2022.03.012.